Presenting Complaint and History
A three-month-old, intact female Miniature Australian Shepherd was presented to MedVet Dallas for hematuria and a distended abdomen. Initial diagnostic tests and results were as follows:
- A complete blood count (CBC) showed neutrophilia and monocytosis.
- Biochemistry profile showed mildly elevated Gamma-Glutamyl Transferase (GGT) and mildly elevated chloride.
- An abdominal ultrasound was performed and showed a large, invasive mass that appeared to be originating from the right kidney.
- Fine needle aspiration (FNA) of the mass was performed and showed the following representative images.
Slides for Evaluation
Review these images from the fine needle aspirate of the abdominal mass (figure 1 -3). Formulate a diagnosis or list of diagnoses based on cytologic findings.
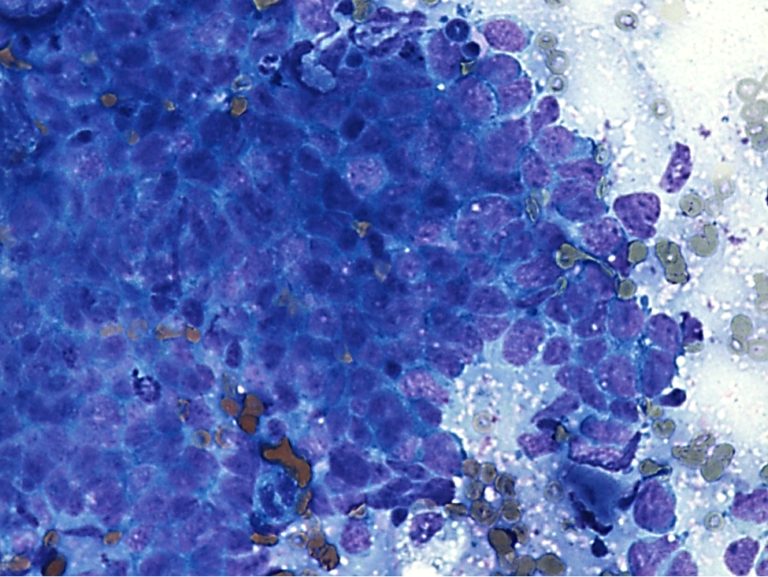
Figure 1. Cytology from an abdominal mass in a puppy. Sheets of atypical cells forming papillary projections. Wright-Giemsa stain. 500x magnification.
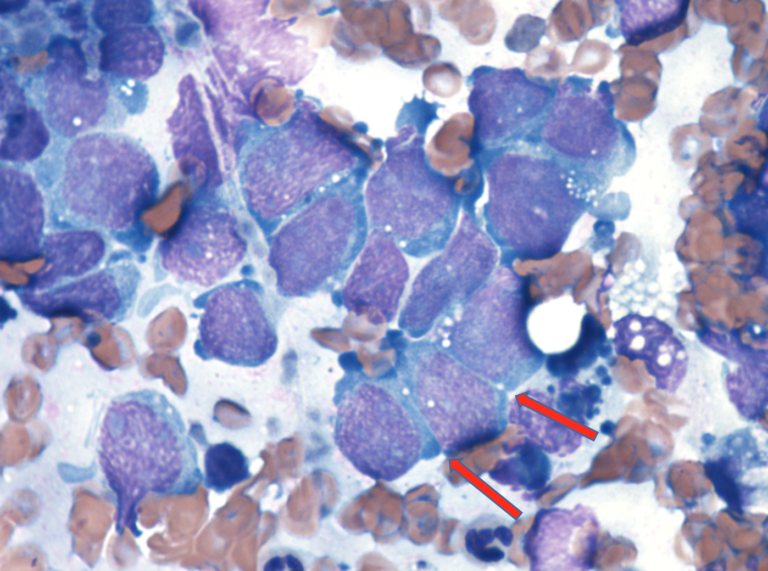
Figure 2. Cytology from an abdominal mass in a puppy. Representative cells with a round to polygonal shape with occasional distinct cytoplasmic junctions (arrows). Wright-Giemsa stain. 1000x magnification.
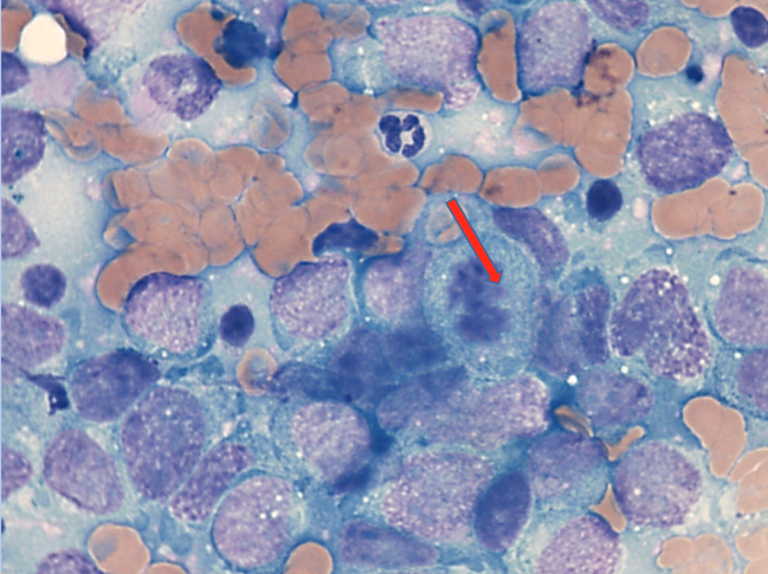
Figure 3. Cytology from a puppy with an abdominal mass. Representative cells with a mitotic figure (arrow). Wright-Giemsa stain. 1000x magnification.
Interpretation
The nucleated cells in the cytologic specimen were composed of clusters and aggregates of atypical cells with variably-distinct cytoplasmic borders. Papillary projections and ribbon formations were seen in the cellular aggregates. The individual cells measured 1.25-2.0x the size of a neutrophil. The cells were rounded to polygonal and had a moderate amount of basophilic cytoplasm containing few small clear vacuoles. Prominent intercellular junctions were noted. Nuclei were round to ovoid, centrally to eccentrically located and have finely granular chromatin containing multiple round nucleoli.
The cells were uninucleate and exhibited mild to moderate anisocytosis and anisokaryosis. There was increased mitotic activity noted within the cell population. Based on the cytologic features, the location of the mass and the young age of the dog, the top differential was a nephroblastoma. A renal carcinoma or renal lymphoma were considered less likely differentials. Biopsy with histopathologic examination was recommended to confirm.
Diagnosis: Renal Nephroblastoma
The patient was taken to surgery. Upon abdominal exploration, a large,invasiveright kidney mass was seen that was engulfing the blood supply to the pancreas and duodenum and was firmly adhered to ileocecal junction. Variably sized, firm nodules were seen throughout the omentum. A 6 cm hepatoduodenal lymph node was also noted. Due to the invasive nature of the mass and suspected metastasis, the patient was euthanized. Histopathology was performed and confirmed nephroblastoma with a predominant epithelial component.
Renal nephroblastoma is a rare tumor that primarily occurs in juvenile dogs. The metastatic rate of these tumors is high in dogs. Cytology and histopathology typically show a “triphasic pattern” of epithelial, mesenchymal, and embryonal glomeruli.
In this case, only the epithelial component was identified cytologically and was the predominant cell type seen on histopathology. A few primitive glomerular structures were seen on histopathology which helped confirm the diagnosis (see figure 4 below).
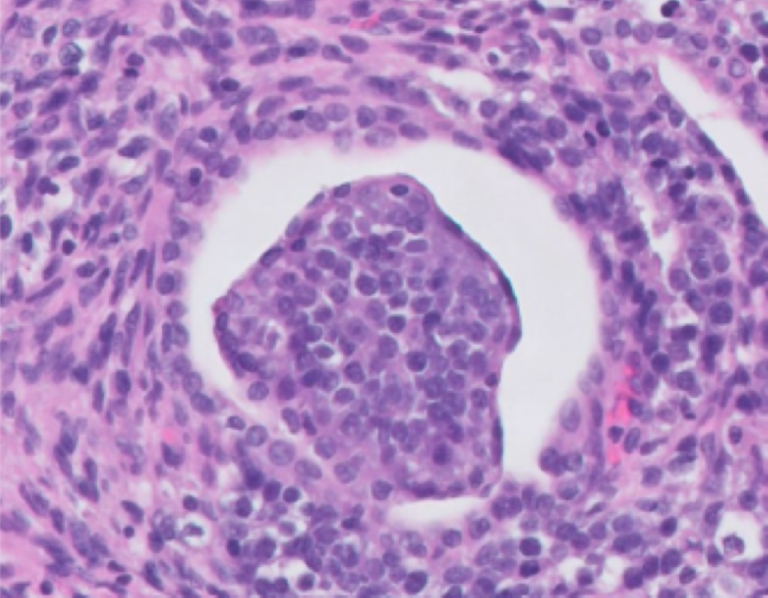
Figure 4. A representative area of the nephroblastoma with a primitive glomerulus.
Cytologically, the epithelial cells in these tumors can sometimes be mistaken for large lymphoid cells, however the papillary projections, prominent intercellular junctions, and lack of lymphoglandular bodies (cytoplasmic fragments of lymphoid cells) helped prioritize a differential of renal nephroblastoma in this patient.
Acknowledgements
*Thank you to Dr. David Gardiner and Dr. Katherine Mix for their contributions to this case report.
