Intervertebral disc disease (IVDD) is a commonly encountered neurological disease of the dog; however, clinical signs within this affected population can be widely variable. With a broad spectrum of clinical presentations, it is important for veterinarians to identify between cases that can be medically managed and those that would benefit from referral. The goal of this article is to provide tools for identifying cases of suspected IVDD and tips for determining when to rest versus when to refer.
IDENTIFYING IVDD
Signalment
IVDD has a reported prevalence of approximately 2% in the canine population. The incidence of this disease increases further in certain breeds with reported prevalence up to 24% in Dachshunds. Other reported breeds at an increased risk for IVDD include the French bulldog, Pekingese, Beagle, Cocker Spaniel, Lhasa Apso, Shih Tzu, Jack Russel Terrier, Bichon Frisé, Maltese, and Miniature Poodle.
IVDD is less frequently diagnosed in large breed as compared to small breed dogs but can commonly occur in mixed breeds, German Shepherds, Labrador Retrievers, Rottweilers, Dalmatians, and Doberman Pinschers. Age of onset can be variable, but it is rare to occur under 2 years of age. There is no sex predilection. IVDD is uncommon in cats, but when it does occur, it tends to be more common in middle aged to older cats affecting the lumbar or thoracolumbar spine.
- Refer rather than rest with:
- Animals presenting with an atypical signalment for IVDD (e.g. young large breed dogs, dogs less than 1 year of age, cats)
History
Clinical history can be highly variable in cases of IVDD in dogs. Onset of clinical signs can be acute or chronic and clinical severity can be static, progressive, or waxing/waning. While the history may do little for narrowing the differential list, it can play a large part in decision making between empirical treatment or pursuing further diagnostics.
- Refer rather than rest with:
- Rapidly worsening weakness or ataxia
- Severe pain or pain unresponsive to oral pain medications
- Weakness, pain, or ataxia persisting > 1-2 weeks despite limited activity
Examination
The purpose of the neurological examination is to determine both the localization and severity of signs. Clinical signs associated with IVDD are non-specific (see Table for a list of differential diagnoses). Referral is recommended for all animals who are presenting as non-ambulatory. While the definition of non-ambulatory varies slightly between neurologists, it typically refers to animals unable to take 3-5 steps unassisted.
- Refer rather than rest with:
- Animals unable to stand/walk without assistance
- Rapidly worsening weakness or worsening despite rest
- Severe pain or pain unresponsive to medications
DIFFERENTIAL DIAGNOSES
IVDD cannot be diagnosed with exam alone. There are several differentials that can present similarly. A list of differentials according to localization are listed below (Table 1).
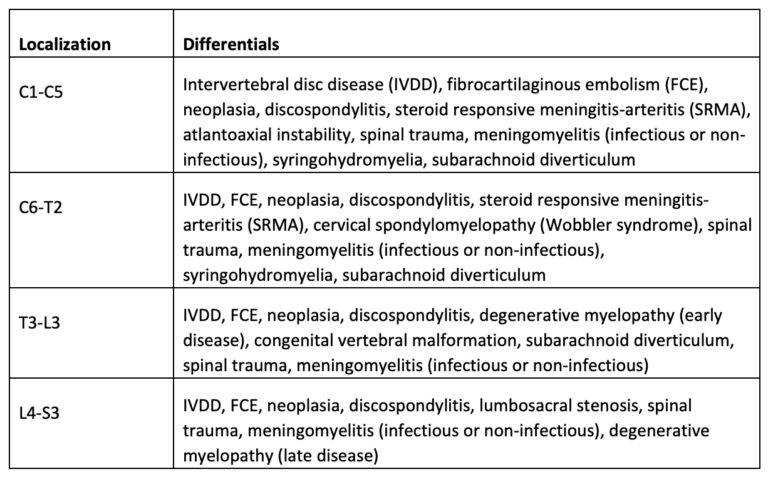
Table 1. List of differential diagnoses in pets with clinical signs of intervertebral disc disease (IVDD) according to localization.
DIAGNOSTIC TESTING PRIOR TO REFERRAL
Many baseline diagnostics can be performed with the primary veterinarian prior to referral. The following is a table (Table 2) outlining diagnostics tests that could be useful in the diagnostic workup of spinal cord disease prior to advanced imaging such as CT or MRI.
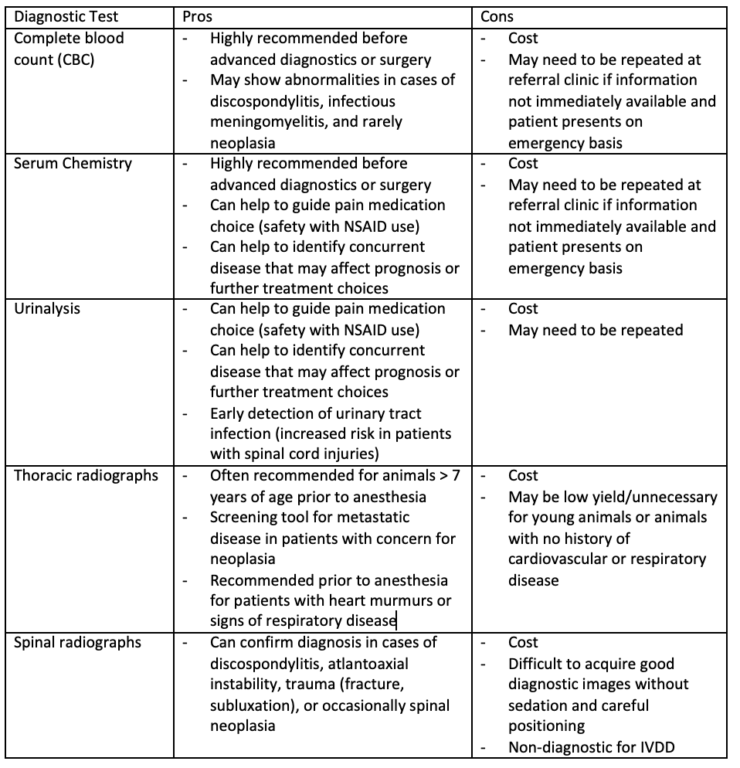
Table 2. Diagnostics tests that could be useful in the diagnostic workup of spinal cord disease prior to advanced imaging such as CT or MRI.
WHEN TO REST AND WHEN TO REFER
The choice whether to pursue medical management or further diagnostics should always be given to the client; however, it is the duty of the veterinarian to guide that decision with clinical reasoning. The following are some scenarios that may help to differentiate those cases that may do well with medical management versus those that would benefit from referral or further diagnostics.
In all cases where medical management is initially pursued, the appropriate follow-up should be in place to quickly identify cases that are failing to respond. Patients that show progression despite rest or fail to improve within 1-2 weeks should have further workup to determine the most appropriate treatment.
Cases that may benefit from medical management alone:
- Age and breed commonly affected by IVDD
- History of back pain, weakness, or ataxia that has previously improved with rest
- Recent onset of clinical signs
- Ambulatory without assistance
- No evidence of rapid progression/worsening of clinical signs following initial onset
Cases that would benefit from referral/further diagnostics:
- Uncommon age/breed for IVDD
- Rapidly worsening weakness or ataxia
- Severe pain or pain unresponsive to oral pain medications
- Weakness, pain, or ataxia persisting > 1-2 weeks despite limited activity
- Animals unable to stand/walk without assistance
