Several skin diseases may affect the nasal planum, or external nose, of dogs. A few of these only affect the nasal planum. An overview of salient features of the more common skin diseases affecting the nasal planum of dogs is presented. The aim is to familiarize one with the clinical appearance of nasal planum diseases, so one can formulate a differential list, work through a diagnostic plan, and prescribe a treatment plan.
The nasal planum has a distinct cobblestone architecture, pigmentation, and a modified thick epidermis characterized by rete pegs and absence of hair follicles. Diseases that affect this anatomic site may be congenital, environmental, infectious, metabolic, immune-mediated, autoimmune, or neoplastic in origin.
Many lesion types occur on the nasal planum. If scale is seen, we consider metabolic conditions like zinc responsive dermatosis, congenital conditions like inherited nasal hyperkeratosis, or early presentations of immune mediated conditions like those in the pemphigus complex. If depigmentation is noted, we differentiate between inflammatory conditions like discoid lupus erythematosus where there is a loss of cobblestone architecture and non-inflammatory conditions like vitiligo where the cobblestone architecture is maintained. If erosions, crusts, and ulcers are noted, we consider infectious, immune mediated, autoimmune, or neoplastic conditions.
Types of Infectious Skin Diseases
Mucocutaneous Pyoderma (MCP)
Mucocutaneous pyoderma (MCP) is a common condition that may affect the nasal planum. MCP is a bacterial infection usually caused by Staphylococcus pseudintermedius. German shepherd dogs are the most commonly affected breed. MCP affects the mucocutaneous junctions of the nasal planum and lips primarily, but other mucocutaneous junction sites are usually concurrently affected. If the nasal planum is affected, there is an initial erythema and swelling of nasal planum, typically at the alar folds. Crusts then fissures and erosions develop. A thick purulent exudate is revealed beneath elevated crusts and one can observe the erosive to ulcerative dermatitis. Diagnosis is made via dermatologic examination, cytology and response to treatment. Cytology of exudate reveals bacteria and inflammatory cells. Bacterial culture and susceptibility testing of revealed purulent exudate from under a protected crust is indicated if there is a failed response to appropriate antibiotic therapy. If cytology does not reveal bacteria, a bacterial culture is sterile, and there is a failed response to antimicrobial therapy, submission of a tissue biopsy for dermatohistopathology is indicated, as Discoid lupus erythematosus is a condition with similar clinical appearance. A fungal culture may also be indicated, as some fungal diseases share clinical features with MCP. Treatment of MCP involves topical therapies and systemic antibiotics. Maintenance topical therapy is recommended for long term control.


MCP Pretreatment and Post Antibiotic Treatment in a German Shepherd Dog
Trichophyton Dermatophytosis
Trichophyton dermatophytosis is one of the most common fungal infections we see affecting the nasal planum in dogs. Its clinical presentation mimics several of the more common diseases. This condition is caused by infection with the soil-borne dermatophyte Trichophyton mentagrophytes. Dogs that hunt or root in soil are at risk. Jack Russell terriers a commonly affected breed. Lesions of the skin and nasal planum may include: alopecia, erythema, papules, scaling, crusting, erosions, or ulcerations. If lesions affect the nasal planum and bridge of nose, the clinical appearance may resemble MCP, Pemphigus foliaceus, Pemphigus erythematosus, dermatomyositis, and other conditions. Pruritus of lesioned sites varies from absent to severe. Diagnosis is accomplished via dermatologic examination, skin scrapings, cytology, culture, and dermatohistopathology. The potential for this infection is the reason to perform tissue fungal cultures and special stains on biopsy samples when working to diagnose diseases of the nasal planum. One does not want to immunosuppress a dog with glucocorticoids if there is a fungal infection. To treat Trichophyton dermatophytosis, systemic and topical antifungal agents are prescribed.

Trichophyton dermatophytosis affecting the muzzle and nasal planum in a dog
Autoimmune and Immune-Mediated Diseases on the Nasal Planum
Discoid Lupus Erythematosus (DLE)
Discoid lupus erythematosus (DLE) is an autoimmune disease that affects the nasal planum of the dog, and is the second most common immune-mediated dermatitis in the species. Ultraviolet light exposure aggravates this condition. Some breeds are overrepresented and include collies, Shetland sheepdogs, Australian shepherds, border collies, German shepherds, and Siberian Huskies. Lesions begin on the nasal planum with loss of pigment resulting in a slate-grey color. Then there is a loss of cobblestone architecture to the nasal planum. With time, lesions develop into erosions and ulcerations. Lesions may extend up the bridge of the muzzle and affect the lips, eyelid margins, and other mucocutaneous sites. Scarring occurs with chronicity. DLE resembles MCP clinically and histologically. DLE resembles some fungal infections clinically. To differentiate between DLE and MCP, it is important to resolve any secondary infection and then biopsy the nasal planum if lesions persist. The pathologist will be able to give a stronger etiologic diagnosis if infection has been resolved. Histologically in DLE there is an interface dermatitis with focal hydropic degeneration of basal cells, pigmentary incontinence, thickening of the basement membrane zone, apoptosis, and perivascular inflammation with monocytes and plasma cells. A preferred initial therapy involves use of 0.1% tacrolimus twice daily that is then tapered over time. Sun avoidance is recommended. Doxycycline or tetracycline in combination with niacinamide may be added. Use of topical glucocorticoids was previously the initial therapy. However, cutaneous changes of scarring and atrophy were common. It is extremely rare to need to deploy use of systemic glucocorticoids for DLE.


Mild DLE in a Collie Pre Treatment and Post Treatment with a Topical Steroid (Synotic)

Severe DLE Pre Treatment
DLE in a Collie Under Treatment with Tacrolimus 0.1%
DLE in a Weimaraner After 3 Weeks of Treatment with Tacrolimus 0.1%
Diseases of the Pemphigus Complex
Diseases of the pemphigus complex may affect the nasal planum. Pemphigus foliaceus (PF) and Pemphigus erythematosus (PE) are the most common. Depigmentation, crusting, and ulceration of the nasal planum together with a crusting dermatitis of the dorsal bridge of the nose can occur in both PF and PE. Lesions of PE are limited to the face, periocular skin, and pinnae. In PF, there is usually a pustular to crusting dermatitis also affecting other body sites including the trunk, ventrum, axillae, pinnae, genitalia and pawpads. Typical breeds include the akita, chow chow, dachshund, bearded collie, Newfoundland, Doberman pinscher, cocker spaniel, Australian sheepdog, and rottweiler. Sun exposure may exacerbate. In PF or PE, autoantibodies are generated against the intercellular assembly holding keratinocytes together. With premature loss of adhesion between keratinocytes, keratinocytes are released. We call these acantholytic cells. Acantholytic cells may be identified cytologically. Other conditions may have acantholytic cells (dermatophytosis, bacterial folliculitis), so one cannot use the identification of acantholytic cells as a sole diagnostic criterion. Dermatohistopathology is the diagnostic test to perform in addition to proving sterility of pustular lesions via bacterial and fungal culture. Histology will show subcorneal to intragranular pustules with acantholytic keratinocytes among a population of neutrophils (some cases have abundant eosinophils). Pustules often span several follicular ostia. Depending on severity and extent, topical therapy may be the only intervention needed for facial limited PE. I treat as for DLE. For more severe cases of PE and for PF, systemic immunosuppressive therapy is needed. The most common initial glucocorticoid used is prednisone. I reevaluate after 2-3 weeks of 2 mg/kg given po q 24 hrs. I monitor a CBC and chemistry profile regularly. Azathioprine is my second drug used. I start azathioprine at 2 mg/kg po q 48 hrs if there has been inadequate lesion resolution on prednisone monotherapy at the early rechecks. Rarely, in severe cases, I start azathioprine and prednisone at the onset of therapy. We are seeing more drug induced cases of PF consequent to topically applied flea and tick control products. The lesion distribution in these cases starts at the site of application of the product and spreads along the dorsum in a drip or saddle pattern. If one is evaluating a crusting dermatitis with such a lesion distribution and such products are used, drug-induced PF should be a differential.

Pemphigus Affecting the Nasal Planum and Bridge of Nose
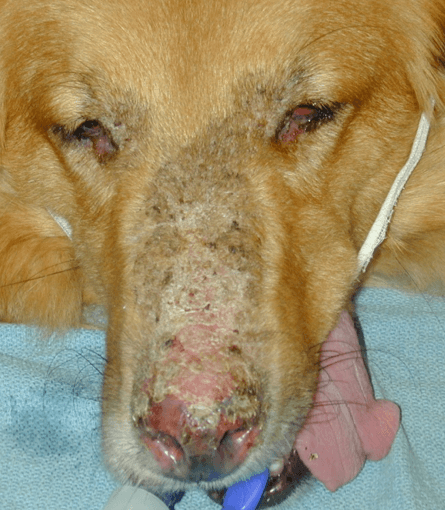
Pemphigus Erythematosus in a Golden Retriever

Pemphigus Affecting the Nasal Planum and Bridge of Nose in an Australian Shepherd

Pemphigus Affecting the Nasal Planum and Bridge of Nose in a Curly Coated Retriever
Cutaneous Reactive Histiocytosis (CRH)
Cutaneous reactive histiocytosis (CRH) may affect the nasal planum. It is a reactive proliferation of activated dermal antigen presenting cells that is thought to a loss of immune regulation caused by some immune system “insult.” Nodular lesions, often forming coalescing clusters are typical. Nodules are cutaneous to subcutaneous, firm, and erythematous. They may resemble urticaria. Some dogs have infiltration of the nasal planum and nasal mucosae causing a clown nose appearance, stridor, and snoring. Collies and Shetland sheepdogs are the most commonly affected breeds. Diagnosis is accomplished via dermatologic examination, aspirate cytology, tissue cultures and dermatohistopathology. Histology shows a nodular to diffuse deep dermal infiltrate of histiocytes that are cytologically normal. Lymphocytes and neutrophils are also present. Special stains are used to look for infectious organisms that cause pyogranulomatous disease. Cell marker studies may be needed to differentiate from other histiocytic diseases (e.g. histiocytic sarcoma). Abdominal ultrasound and thoracic radiographs may be helpful to rule out systemic histiocytic disease. Treatment of CRH involves glucocorticoids, tetracycline or doxycycline and niacinamide, cyclosporine, or leflunomide.


Cutaneous Reactive Histiocytosis Affecting the Nasal Planum of a Dog
Uveodermatologic Syndrome
Uveodermatologic syndrome is a rare immune-mediated disorder that may affect the nasal planum. It is caused by cell-mediated hypersensitivity to melanocyte antigens. This disease is most commonly seen in Siberian huskies, Akitas, Samoyeds, and Chow Chows. The first sign is typically a granulomatous uveitis that can result in blindness if not treated early and aggressively. Skin lesions usually develop after the uveitis, and are characterized first by depigmentation of the nasal planum, lips, and/or eyelids. Thereafter, erythema, erosions or ulcers, and crusting occur. The diagnosis is accomplished via signalment, history, and dermatohistopathology. Treatment involves immunosuppression most commonly with glucocorticoids and azathioprine in addition to ophthalmic medications.
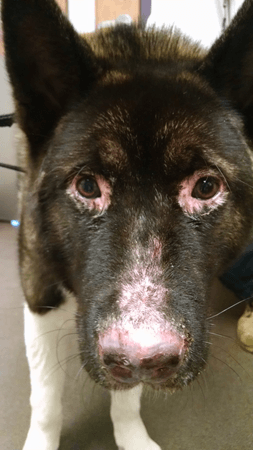
Uveodermatologic Syndrome Affecting the Nasal Planum of a 1-year-old Male Akita
Vitilogo
Vitiligo may affect the nasal planum. It is an immune-mediated destruction of the melanocytes. Lesions are characterized by leukoderma (loss of pigment in the skin) and/or leukotricia (loss of pigment in the hair). Rottweilers, doberman pinschers, collies, and giant schnauzers are most commonly affected. The depigmentation often occurs on the nasal planum, but the lips, and periocular skin are often involved. Leukoderma and leukotricia may ultimately involve large areas of the body. On the nasal planum, there is depigmentation with retention of the cobblestone architecture. Erosions, ulcers, crust are absent. Uveodermatologic syndrome can start in this manner, so a thorough ophthalmic examination is recommended. Diagnosis is accomplished by history, signalment, dermatologic examination and dermatohistopathology. This is a cosmetic disease. No treatment is prescribed. Sun avoidance is recommended, so there is less risk for future ultraviolet induced skin conditions.

Vitiligo Affecting the Nasal Planum, Skin, and Hair
Keratinization Disorders on the Nasal Planum
Nasal Hyperkeratosis
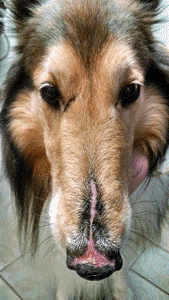
Nasal Hyperkeratosis is an idiopathic condition that may affect the nasal planum of older dogs. The American cocker spaniel and the English bulldog are over represented. There is marked hyperkeratosis with excessive fronding of the dorsal nasal planum adjacent to haired skin. The pawpads may be affected by similar hyperkeratosis and fronding. This is a cosmetic disease. However, if it is severe enough to cause fissures, secondary bacterial infections may occur. Diagnosis is accomplished by signalment, history and dermatologic examination. Treatment involves topical keratolytic agents with salicylic acid or other moisturizing ointments. Most recently I have been using Dermoscent Biobalm® (Bayer Animal Health) with success.
Hereditary Nasal Parakeratosis of the Labrador Retriever
Hereditary Nasal Parakeratosis of the Labrador Retrieveris an autosomal recessive trait resulting in a keratinization defect of the nasal planum. It affects Labrador retrievers. Onset is noted at 6-12 months of age. There is dorsal nasal planum hyperkeratosis that is gray-brown in color. Diagnosis is made based upon signalment, history, and dermatohistopathology. Histology reveals parakeratotic hyperkeratosis with intercellular fluid (serum lakes). I treat as for nasal hyperkeratosis of older dogs, and most often use Dermoscent Biobalm® (Bayer Animal Health) twice daily to effect and maintain use a few times per week.

Hereditary Nasal Parakeratosis of the Labrador retriever
Neoplastic Diseases on the Nasal Planum
Squamous Cell Carcinoma (SCC)
Squamous Cell Carcinoma (SCC) is the most common neoplasia of the nasal planum. SCC may develop due to actinic damage in lightly pigmented breeds, in association with chronic inflammation (DLE, MCP, PF, reactive histiocytosis), or may be spontaneous. Certain breeds are more at risk including the Scottish terrier, Pekingese, boxer, poodle, and Norwegian elkhound.

Squamous Cell Carcinoma of the Nasal Planum in a Border Collie
Cutaneous T-cell Lymphoma (CTCL)
Cutaneous T-cell Lymphoma(CTCL) can affect the nasal planum. Lesions include depigmentation, erosions and ulcers. CTCL is considered the “great imitator,” as lesions can mimic pruritic, immune-mediated, autoimmune, or keratinization diseases. If there is nasal depigmentation in an older dog, CTCL should be a differential. The nasal planum may be the only affected site, but lips, other mucus membrane sites, and haired skin may be lesional. Diagnosis is accomplished via dermatohistopathology +/- immunohistochemistry. Bacterial and fungal cultures are recommended to rule-out infectious causes. Histology shows epitheliotrophic lymphocytes that have atypical features. There may be band of pleomorphic lymphocytes in the superficial dermis (lichenoid band). Treatment may involve Lomustine, prednisone, and nutroceutical therapies.



Cutaneous T-cell Lymphoma in a Beagle and a Boxer
Diseases of Unknown Cause on the Nasal Planum
Nasal Hypopigmentation/Nasal Depigmentation
Nasal hypopigmentation/Nasal depigmentation is a condition of depigmentation limited to the nasal planum. It is often called “Dudley nose.” Dogs are born with normal pigmentation of the nasal planum, and have a gradual fading of color during the first few years of life. It may be a form of vitiligo. It has been noted in the Afghan hound, Samoyed, Siberian husky, yellow Labrador retriever, white German shepherd, golden retriever, poodle, Doberman pinscher, and Irish setter. This is a permanent depigmentation. A seasonal depigmenting condition called “Snow nose” has been noted in Siberian huskies, Labrador and Golden retrievers, and Bernese Mountain dogs. There is a cyclical loss of pigment during the winter months with repigmentation in the spring and summer.

Nasal Depigmentation (“Dudley nose”) in a Golden Retriever
Dermal Arteritis of the Nasal Philtrum
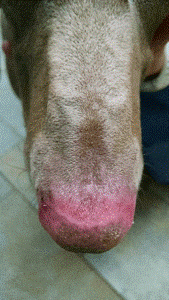
Dermal arteritis of the nasal philtrumis a rare disease that affects a specific anatomic site of the nasal planum. It has been identified in large breed dogs such as Saint bernard, giant chsnauzer, and great dane. It affects the large arteries and arterioles of the central aspect of the nasal philtrum. Lesions are solitary circumscribed erosions and ulcers. Lesions often bleed and bleeding may be profuse. Onset is noted at 3-6 years of age. The cause is unknown. Diagnosis is made via history, signalment, examination, and dermatohistopathology. Histology of deep arteries and arterioles will demonstrate proliferative arteritis with intimal cell proliferation and stenosis. Treatment includes topical and systemic glucocorticoids. I have had one dog require surgical intervention due to profuse recurrent bleeding from the nasal philtrum.

