Guide to the Diagnosis and Treatment of Vestibular Dysfunction in Dogs and Cats
Disorders of the vestibular system are commonly encountered in domestic species of dogs and cats. Proper diagnosis is key to successful treatment, with most forms of vestibular disease being treatable. Diagnosis can be aided by the history obtained from the client, as well as careful examination of the vestibular system. Diagnostic testing may further support and/or confirm a diagnosis, leading to definitive treatment options.
The ultimate goals of the clinician regarding vestibular dysfunction is to recognize the presence of a vestibular problem and attempt to classify the lesion as peripheral or central.
The following are signs seen with vestibular dysfunction:
Signs of Vestibular Disease in Dogs and Cats
Generic vestibular signs:
- Ataxia
- Head tilt
- Pathologic nystagmus
- Strabismus
Other signs:
- Tachycardia
- Ptyalism
- Vomiting
- Inappropriate urination/defecation
The following signs are typically seen with peripheral disease:
Peripheral – Unilateral:
- Head tilt toward lesion
- Pathologic jerk nystagmus
- Positional or sustained – make sure to place patient on their back
- Fast phase – directed away from the lesion
- Asymmetric ataxia
- Ipsilateral facial weakness
- Strength preserved
- Normal proprioception – Only in patients able to stand; you may have to wait 24 hours, then reassess
Peripheral – Bilateral:
- Bilaterally wide head excursions (serpentine head movements)
- Head tilt may be absent
- +/- Nystagmus
- Crouching posture
- Bilateral facial weakness
- Strength preserved
- Normal proprioception – Only in patients able to stand; you may have to wait 24 hours, then reassess
Central disorders are those which involve vestibular structures located within the caudal fossa. The most reliable indicator of central vestibular dysfunction are other neurologic deficits.
Central:
- Delayed/absent postural reactions
- Other cranial nerve deficits
- Weakness
- Not to be confused with imbalance
Paradoxical vestibular disease:
- A unique central disorder
- Head tilt and loss of balance opposite side of lesion
- Nystagmus toward lesion
- Side of lesion is determined by side of postural deficits, other CN deficits and/or hemiparesis
Table 1. Comparison of peripheral and central vestibular signs/symptoms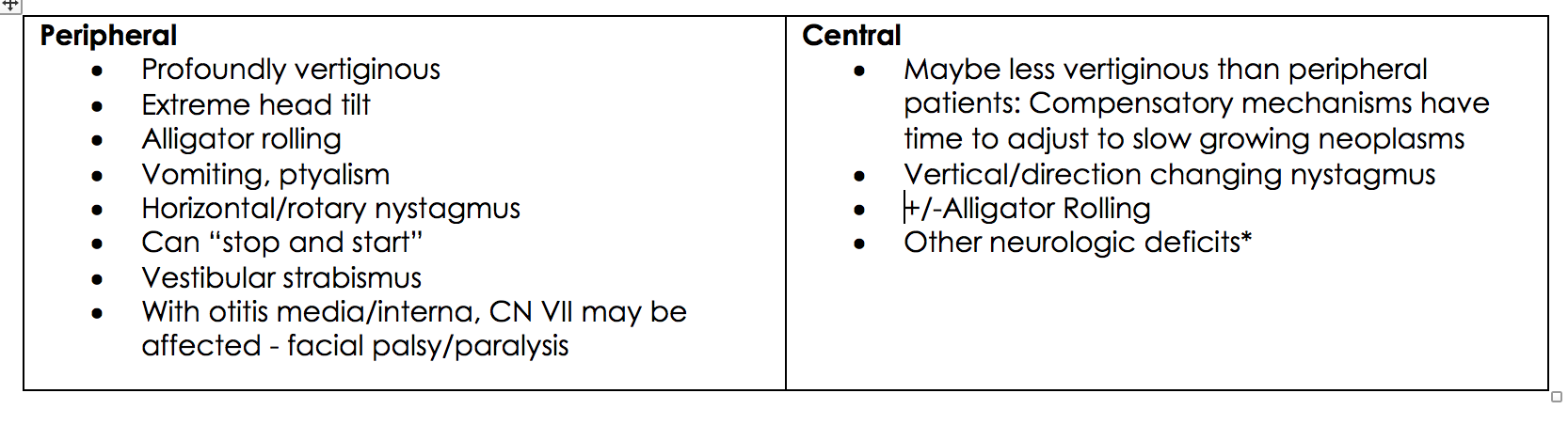
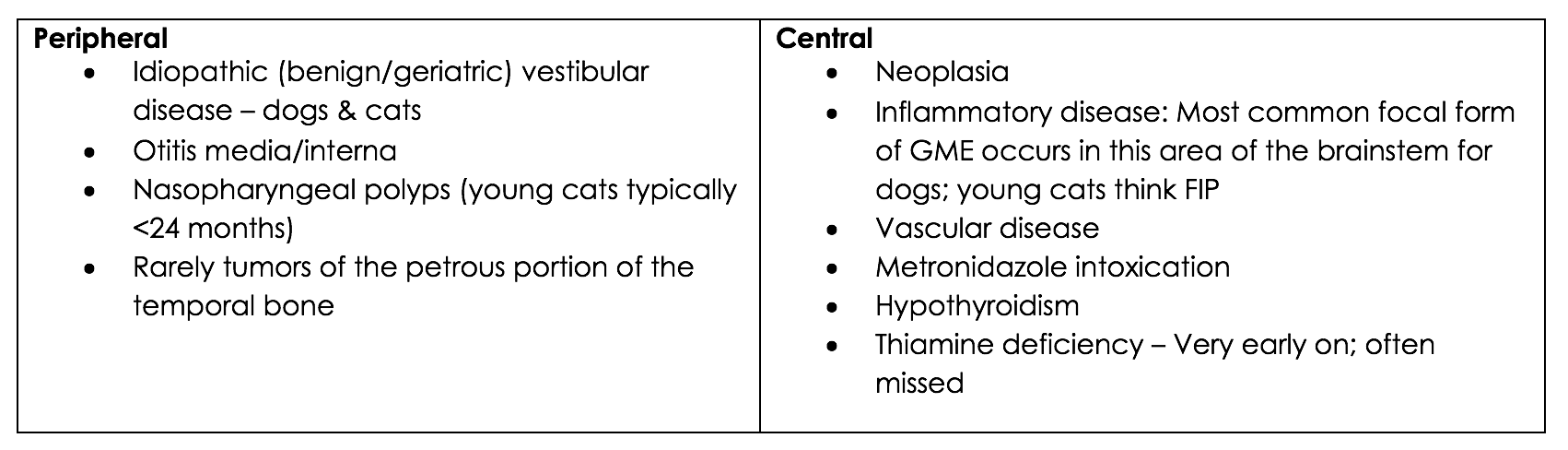
Table 2. Differential diagnoses for vestibular disease in dogs and cats
Congenital Disorders:
- Vestibular disease
- Clinical signs present at birth or when patient first walks
- May improve/recover
- Congenital Nystagmus:
- Pendular
- No fast phase: equal velocity to both sides
- Benign
- May spontaneously resolve
Additional Notes:
- With time general proprioception and vision will compensate for balance
- At night patients may be more vertiginous – leave a light on!
- With acute onset, severe disease can be debilitating, but very often recoverable
Diagnosis of Vestibular Disease in Dogs and Cats
Clinical Approach to Diagnosis:
- Is the patient displaying symptoms of vestibular dysfunction (seizures)?
- Severely vertiginous patients may need sedation and time before examination
- History is key! – Duration, progression, degree of imbalance
Diagnostics (as indicated):
- Otoscopic examination – if possible
- Oral examination – especially in cats
- CBC
- Biochemistry panel
- T4/fT4
- Clotting times
- Urinalysis
- Thoracic radiographs
- Abdominal radiographs
Treatment of Vestibular Disease in Dogs and Cats
Therapeutic Options:
Sedation PRN:
Diazepam: 0.25-0.5 mg/kg (q30 min x 2 doses, then CRI at 0.25 mg/kg/min)
Acepromazine: 0.01-0.2 mg/kg q4-6H prn (3 mg total dose)
Additional medications:
Maropitant: 1 mg/kg SQ q24h or 2 mg/kg PO q24h
Meclizine:
Dogs: 0 – 5kg 6.25 mg PO q8-24h
6 – 20kg 12.5 mg PO q8-24h
20kg+ 25 mg PO q8-24h
Cats: 6.25 mg PO q8-24h
Supportive care:
Hospitalization is always recommended for patients who are not drinking, as dehydration from sensible/insensible loss can be profound. Additional care may include:
- Padded cage
- IV Fluids
- Music – “Through a dog’s ear”/quiet environment
Prognosis for Vestibular Disease
The severity of signs does not correlate to prognosis.Many patients will be significantly improved within 48 hours regardless of etiology (improvement may not be sustained).
- Quite favorable as many causes are treatable/manageable
- Recurrence is possible and dependent upon etiology
- If a tumor is suspected, prognosis for 1-year survivability with good quality of life is fair
- Central disease ≠ bad prognosis
